


Global Coronavirus Research: Connections between the Spread of COVID-19 and Japanese Culture
Adam Acar, PhD
Kimono Tea Ceremony Kyoto Maikoya, Gion Geisha Museum, Samurai & Ninja Museum Kyoto
ABSTRACT
Our literature review indicated that during the last two major pandemics, Southern European countries suffered disproportionately more casualties while East Asian nations had lower rates of deaths. To address this phenomenon, we investigated if there are any relationships between cultural, demographic, societal and biological factors and coronavirus cases worldwide. The findings indicated that warm countries are less likely to report coronavirus cases while countries with high male obesity, urbanity, and median age are more likely to face COVID-19 related fatalities.We concluded that Japan’s low number of cases and fatalities could be explained by high levels of hygiene practices, low individual autonomy, high humane orientation, the “low-contact” culture, high internet penetration, low body mass and a high number of hospital beds per capita. We also observed that countries with a higher percentage of blood type O were more likely to report coronavirus fatalities while the opposite was true for the blood type B. Directions for future research provided.
To cite this article: Acar, A (2020). Global Coronavirus Research: Connection between the Spread of COVID-19 and Japanese Culture. To be published in the upcoming issue of the International Journal of Web Based Communities. Retrieved online from https://mai-ko.com/japanese-culture/global-coronavirus-research-connection-between-the-spread-of-covid-19-and-japanese-culture/
Summary of this study is explained by the author in this video
INTRODUCTION
About 102 years ago, a flu-like illness emerged in China () and killed more than 100 million worldwide () . Also known as the Spanish flu, this disease had relatively higher mortality rates in Southern Europe while lower ratios of deaths were reported in Japan, Taiwan, Hong Kong and China () () () . A similar pattern emerged in 2009 during the H1N1 pandemic () where the death rate seemed to be lower for East Asians and higher for Europeans. Nowadays we are witnessing yet another global threat, coronavirus, that is following a similar path (). The current situation begs the question of whether Japanese culture plays a role in the spread of epidemics. This study aims to find an answer by looking at country-wide cultural index scores and mortality rates. The analyses also include demographic, biological and social factors to compare the size of the relationships.
Coronavirus means a crown-shaped virus used to identify a specific group of RNA viruses that cause diseases in humans and animals. The name comes from “corona” in Latin which means crown, a reference to the appearance of the protein particles that cover the main virus cell like the gems on a crown (). The Novel Coronavirus, also known as, Cov, NCov,SARS-CoV-2,2019-nCoV, first emerged in Wuhan, China in December 2019 and soon spread to the rest of the world. In some cases the infections cause severe acute respiratory syndrome called COVID-19 disease which so far has sickened approximately 2 million people and killed more than 125,000 worldwide () .
The UN secretary called the coronavirus pandemic the most severe crisis facing humanity since World War II () and the British prime minister labeled it as the biggest threat () only a few days before he was accepted to intensive care for the infection. Many countries introduced emergency laws and large-scale lock-downs as a social distancing measure to slow down the epidemic which had many economic implications. The Dow Jones Index suffered the largest one-day point drop ever () and the US goverment reported the highest ever monthly unemployment rate increase ever () . A number of companies in the hospitality and tourism industry went bankrupt. 97% of the peak season reservations at Tea Ceremony Maikoya Kyoto, where the lead author of this study works, were cancelled.
Interestingly, South European countries had the largest number of fatalities per million people compared to East Asian countries with Confucius values having the fewest () similar to the Swine Flue outbreak (). What is more, even though East Asian countries followed different epidemic control measures, the results were similar (), which means there may be some sort of cultural or genetic influence on how diseases spread. This study looked at the relationship between cultural index scores, blood types and the number of coronavirus cases and fatality rates to see if there is any pattern.
There were also many intriguing news stories in the mainstream media such as “coronavirus usually spreads through touching paper money” (), “smokers are more likely to catch the disease” () and “countries with mandatory BCG vaccinations are less likely to suffer from Coronavirus” (). Some news reports mentioned that in countries with female leaders, the virus was less likely to spread (). To have a holistic view and approach the issue from different perspectives, we also looked at how nationwide statistics relate to the outcome of countrywide coronavirus infections.
LITERATURE REVIEW
Past Studies on COVID-19
It is also well known that most of the coronavirus patients tend to be male who are older than 40 and had preexisting conditions of diabetes or high blood pressure (). Some early reports suggested that people with Blood Type A usually have the highest risk of getting the COVID-19 disease while the blood type O had the lowest risk (). A study with the sample size of 40 found that the disease causes RNAaemia, acute cardiac injury in addition to the acute respiratory distress syndrome (). A recent news report indicated that African-Americans are significantly more likely to die from the disease compared to Caucasians ().
Culture and Epidemics
Although vastly overlooked, culture and reactions to epidemics seem to be closely related. As the matter of fact, culture itself evolves based on traumatic societal experiences. For instance after the Bubonic plague in the 14th century, a.k.a. Black Death, public hot baths disappeared because people believed warm water opened their pores for viruses to penetrate in (). Vernacular literature emerged and how Europeans viewed religion dramatically changed that led to the Reform and Renaissance ().
More than the social perception of personally transmitted diseases, culture influences how people recognize initial symptoms, take care of themselves, search for help and label those who are infected (). The effect of local customs and social norms becomes even stronger when the epidemic is a sexually transmitted disease, e.g. HIV, because of potential stigmas, or a direct-contact-risk disease, e.g. ebola, because of established cultural burial rituals (). Local cultural values can also play a positive role fighting against epidemics when it comes to taking care of others and self-sacrificing ().
Culture and Social Distancing
Famous cross-cultural researcher Edward Hall coined the term proxemics which deals with the use of space in different cultures. Edward Hall stated that Americans tend to stand 3.6 meters away from acquaintances and 7.6 meters away from strangers (). He also suggested that South Europeans, South Americans and Middle Easterners have “high contact” cultures as they stand closer and touch more whereas Asians, North Americans and Northern Europeans have “low-contact” cultures (). These propositions were recently supported by a large scale cross-cultural study: however, it was found that in general females and the elderly stand further away from others compared to males () regardless of culture. The same study also detected a positive relationship between cold climates and social distance where people in warm countries stand closer. The authors () stated that:
…This relationship offers an alternative, competing hypothesis on temperature–distance association that would include the indirect effect temperature has on interpersonal distance. Many diseases can spread by a simple touch (Schweon, Edmonds, Kirk, Rowland, & Acosta, 2013), and a recent study showed that people were able to detect some infection cues in the body odor of others—this early innate immune response altered the pleasantness of body odor samples (Olsson et al., 2014). Reduction of interpersonal contacts or increasing the interpersonal distance has for centuries been a part of behavioral adaptation against epidemics (Fenichel, 2013), and in regions that have historically suffered from high levels of infectious diseases, people are indeed less extraverted and open (Schaller & Murray, 2008). (pp. 580, Sorokowska et al.)
Culture and Testing
The World Health Organization has been strongly recommending rapid and expansive testing of potential cases in order to monitor and control epidemics (). However, not all countries may want to implement these tests because of practical and cultural reasons. For instance it is proposed that Japanese government discouraged all kinds of tests to be able to create a “safe” image for the Olympics () and China misrepresented the number of cases to jumpstart its economy right away (). Additionally it is believed that testing does not cure the problem () and may make it more difficult to treat patients with an urgent need. A right wing newspaper even claimed that China purposefully sends faulty testing kits to other countries that are not reliable ().
Individuals may also be totally fine with the lack of testing because of the existing decision making patterns in different parts of the world. For instance, American managers in general make more data driven and analytical decisions whereas Japanese managers tend to make decisions that prioritize long term outcomes and tertiary relationships (). While Western culture revolves around positivism, logical bottom-up decision making based on the observation and measurement of our environment, Japanese culture emphasizes the holistic view of the universe and intuitive knowledge (). In the same vein, Western culture teaches us the importance of taking care of ourselves on our own “now” and controlling our environment, whereas Eastern culture focuses on living in harmony with the environment and trusting the authority (). It is not a coincidence that after the Fukushima Earthquake most Japanese did not bother to track the radiation levels while a number of foreigners in Japan launched online radiation databases ().
Culture and Surgical Mask Wearing
For most Westerners, surgical mask-wearing in public used to be perceived strange, something they associated with Michael Jackson (). Japanese, on the other hand, routinely wore surgical masks in public and considered the mask wearers as considerate and socially responsible. While the reasons range from protection from the hay fewer to hiding a face without a make up, research shows that masks in Japan were originally introduced and promoted to stop the Spanish Influenza in 1918 and Italian Flu in 1949 (). It was very popular during the H1N1 outbreak in 2009 (). Even though almost all governments forced the practice of mask wearing during the modern-era pandemics, the behavior somehow became a norm in Japan but disappeared in Western countries. Japanese people wear a mask to not only protect themselves but also protect others and consider it to be a risk ritual that is the collective disempowerment during the times of uncertainty ().
Studies show that surgical masks are also common in other East Asian countries () and associated with effective hygiene practices such as hand washing, gargling and avoiding close contact with infected people (). After the coronavirus outbreak, the WHO recommended against wearing surgical masks for healthy individuals () probably to prevent shortages for the medical personnel and create a false sense of security. However, other Asian countries’ public statements about mask wearing were supportive and definitely not discouraging (). It is also important to note that for the citizens of countries where mask-wearing is uncommon, wearing a mask may not reduce the risk as the wearer may often touch his/her face because of discomfort.
Culture and Hygiene
Currently what CDC () recommends to protect against COVID-19 is mostly related to hygiene (washing hands, disinfecting surfaces, etc.). However, hygiene has a lot to do with culture. For instance a Gallup poll () shows that members of the muslim countries in Europe almost always wash their hands after using the restroom while only about a little more than half the population in South Europe follow this routine. Similarly, Japanese clean their bodies and neighborhoods probably more than other nations () which may be related to the Shinto belief in Japan that everything must be pure both inside and outside. Historic records show that even in the 1500s the Japanese used to take a shower everyday () which was very different from Europe where public baths were discouraged after the “Black Death.” It is suggested that the reason most Portuguese and Spaniards used to be called “Southern Barbarians: nanbanjin” in Japan was that they refused to take a bath often () as they believed hot baths would open their pores for viruses to enter.
Genetics Over Culture
Japanese Culture may fail to explain the spread of epidemics as there are likely to be many other factors such as genetics and biological predispositions to certain diseases. For instance, East Asians in general are less likely to develop tobacco-related lung cancer compared to Caucasians (). During the 2009 H1N1 epidemic, a lower percentage of Asians compared to Europeans died as a result of the way IFITM3 gene functions in East Asian populations (). Similarly, when it comes to obesity and the obesity effect on Type 2 Diabetes, the genes of East Asians influence the human body in a totally different way compared to Caucasians ().
METHODOLOGY
The coronavirus infection rates, cases and fatalities were retrieved from the online Worldometer database () on April 13, 2018. Worldometer is a for profit database managed by an international team of developers that uses publicly available data sources and reportedly have been trusted by ALA, the government of the United Kingdom and The New York Times (). The database is refreshed every 24 hours. Our comparison of the worldometer data numbers were very similar to the John Hopkins University’s database () and the Our World in Data database (), but not exactly the same, which may be related to technical issues or the time of refreshing.
Cultural index variables including Hofstede’s cross-cultural value index, the GLOBE dimensions, the World Values Survey, Trompenaar’s dimensions, Schwartz’ dimensions and Edward Hall’s high context vs. Low context categorization were adapted from the lead author’s study on global social media use and suicide study (). We also included the big 5 personality distributions, self esteem and emotional experience for this analysis. The data sources can be found in the references section of this paper and the explanations can be found in this past study ().
Demographic variables for each country were retrieved from the Worldbank () and Our World in Data () databases.The disease information per country was adapted from the WHO’s “Global Health Observatory Metadata” () and the database of “Our world in data” ().Since the lead author used the some of the data that was mostly put together in his 2014 study, some of the numbers may have been outdated.
The analyses were rather simple since this is a hastily done study to provide some qualitative insights into an ongoing epidemic. An exploratory Pearson correlation analyses were conducted between all the variables followed by data plots generated by IBM SPSS by selecting the countries with the annual avg. temperature lower than 15 C degrees or the OECD countries (to lessen the noise in the graphs). In many analyses the sample sizes may differ which may confuse the readers (e.g. blood type analysis vs. paper money analysis) because most of the data were collected from different sources with incomplete values. For the missing data we used the pairwise deletion.
FINDINGS
Before looking at the effects of culture, we explored the relationships between coronavirus fatalities and demographic and biological factors. Our initial analysis has shown that there was a negative correlation between the annual temperature and the number of coronavirus deaths per 1 Million people death/population (r=-22, p<.05, N=121). After this initial finding we limited the rest of the analyses by excluding warm countries and mostly focused on the OECD countries.
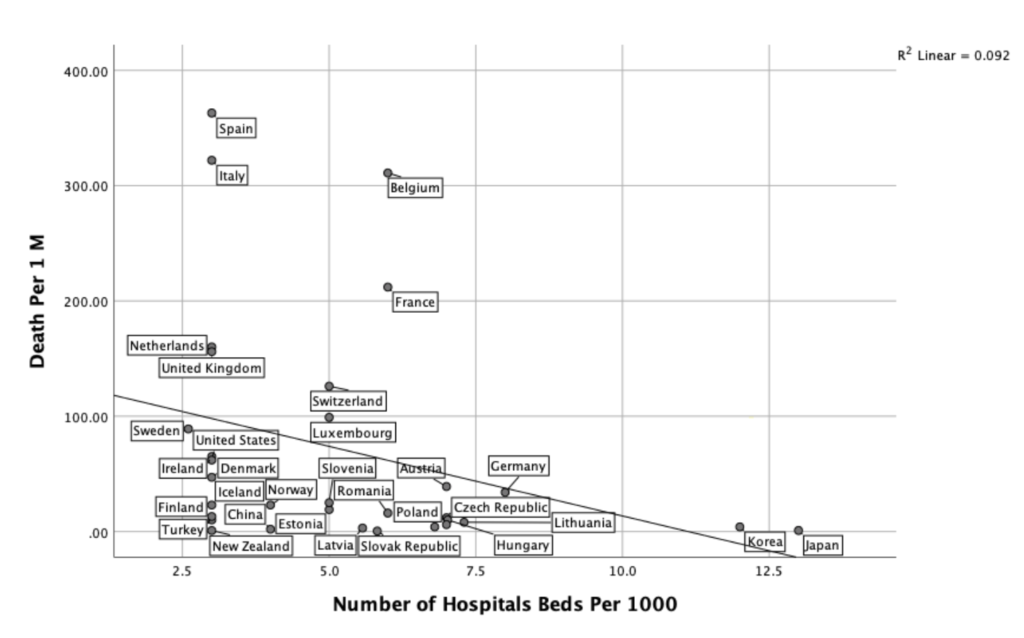
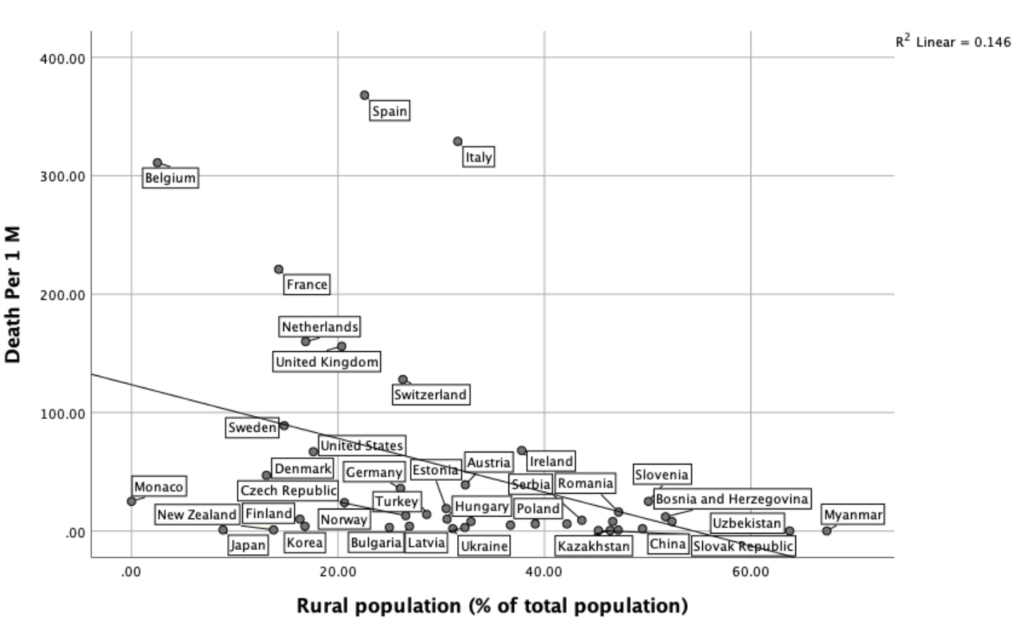
Based on the past literature, we suspected that the quality of the local healthcare system, median age and body mass index are likely to influence COVID-19 fatalities which are most of the time related to the clogging of the medical facilities, percentage of the elderly in the area and the preexisting medical conditions. There was a negative correlation between the number of hospitals per 1000 people and the coronavirus death rate per million people approaching significance (r(32)=-30, p<.1, N=32). We also observed a significant negative relationship between the percentage of rural population and coronavirus fatalities. This means countries with a higher percentage of urban population obviously experiences more medical facility issues or the virus spread more in urban areas.

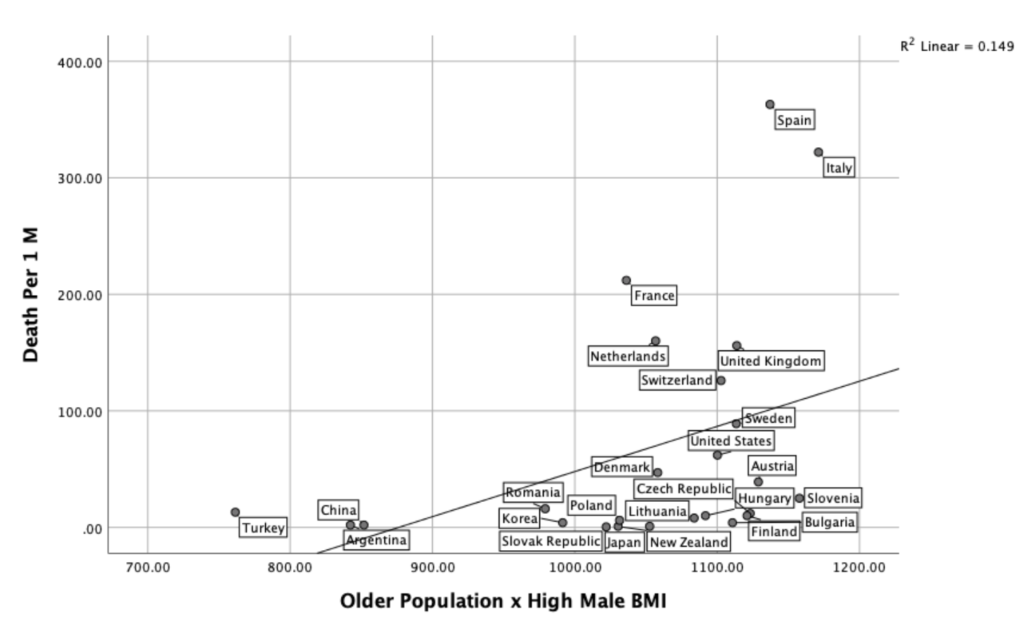
Median age and Body Mass Index were not significantly associated with deaths. However, when we created an interaction variable (AGE x Male BMI), we found that the relationship was almost significant (r(23)=37, p<.1). In other words, in societies with a higher number of hospital beds, fewer people are likely to die from Coronavirus. In societies with older populations and higher male obesity, more people are likely die from Coronavirus.

We could not, however, find significant results after analyzing the US states’ data () regarding the relationship between hospital beds per capita and coronavirus deaths. This may be because we did not have the city-level hospital beds data. The US has 50 states but more than half the deaths so far occurred in the New York-New Jersey metropolitan area (). Additionally, we observed a negative relationship between the rural population and the fatalities which suggests in rural areas the disease is less likely to spread or the cases are less likely to clog healthcare systems.

Cultural Factors
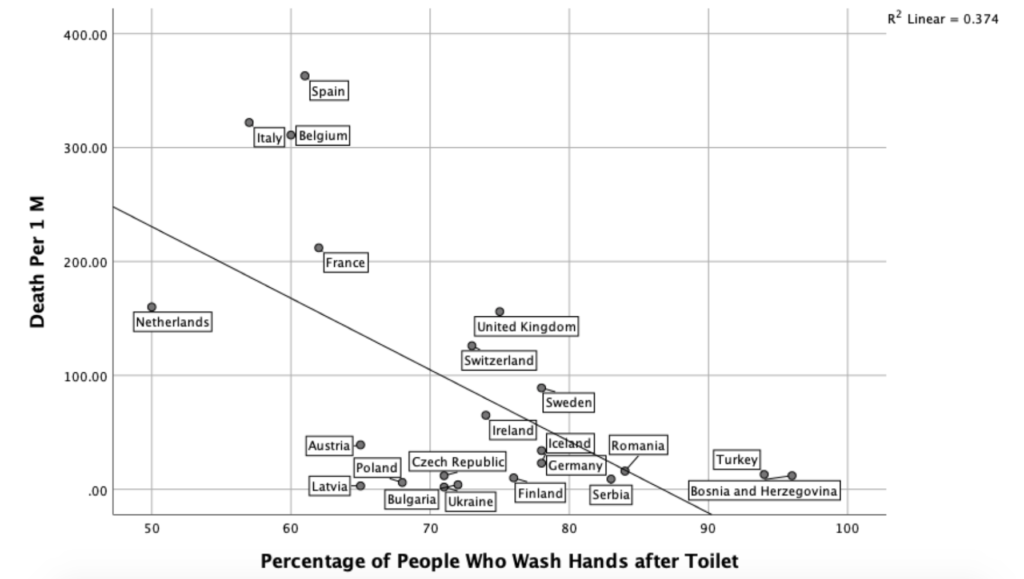
As hygiene is very important for the prevention of epidemics, we wanted to correlate overall hygiene practices and the Coronavirus deaths. Regarding sanitation, cleaning and hygiene behavior we could only retrieve the partially available Gallup Poll results from 2015 () about the hand washing habits after using a restroom. The correlation between handwashing and the number of Coronavirus cases was rather low. However, our analysis showed that there was a clear negative relationship between hand washing after the restroom and Coronavirus deaths (r (22)=-61, p<.05), at least in Europe.

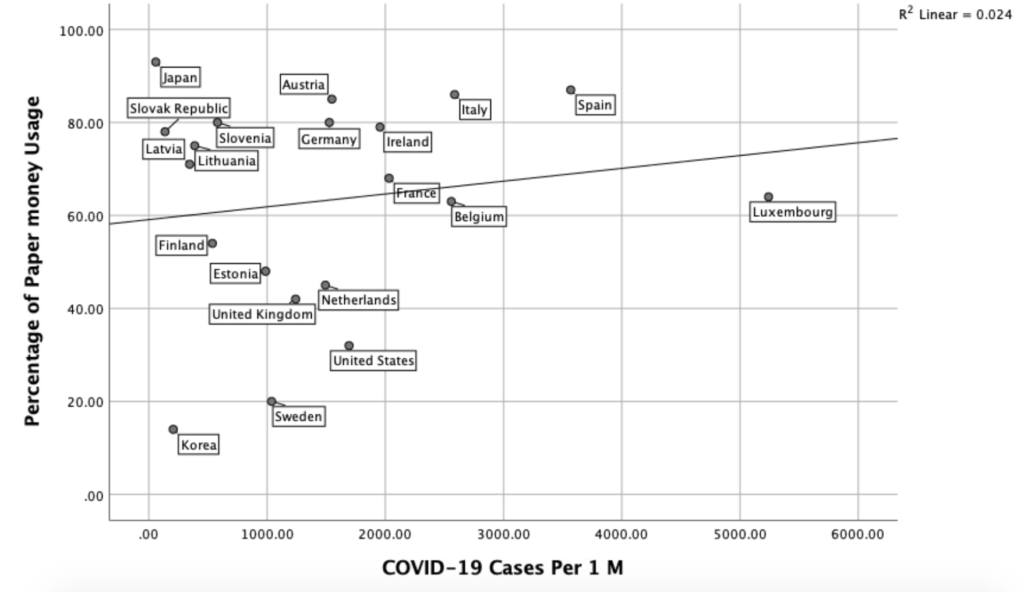
We also looked at the relationship between using paper money and Coronavirus deaths. Recently some news outlets reported public concerns about the use of paper money as paper bills are considered to be less hygienic than credit cards or simply the digital money. We found no significant relationship between coronavirus deaths and the prevalence of using cash though this doesn’t mean paper money is equally clean in every country (e.g. Although Japan has one of the highest rates of using paper money, many Japan visitors are surprised how clean and crisp () the paper bills are).

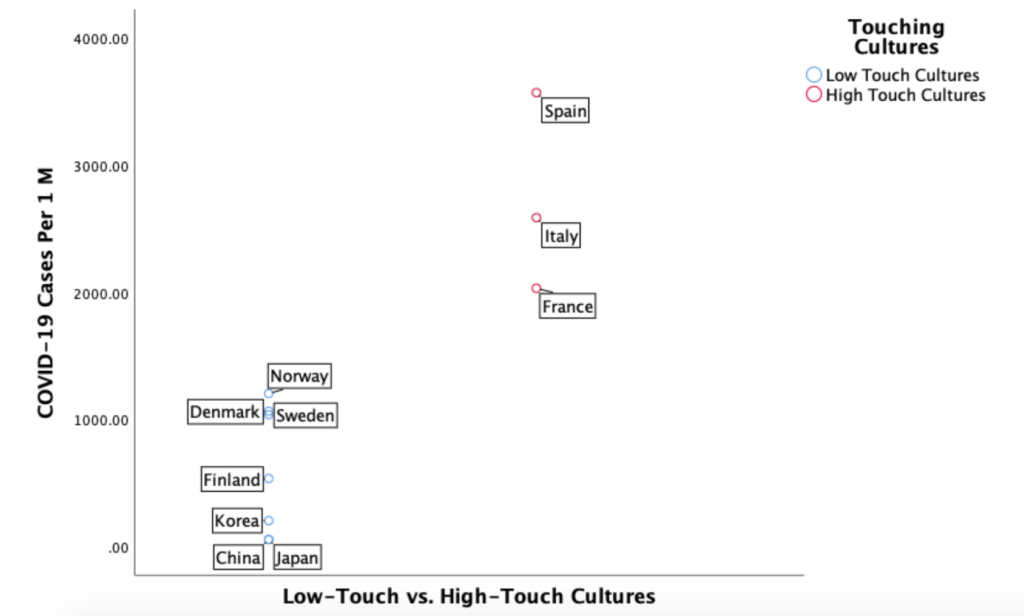
This study also looked at the relationship between the tendency of “touching” in each culture and coronavirus cases. By grouping countries as high-touch or low-touch based on Hall’s judgment (), we found that countries that have the touching culture are significantly more likely to report higher coronavirus cases and higher coronavirus deaths compared to non-touching cultures. Some South European countries (e.g. Portugal, Greece) are excluded in this graph because they have an avg. annual temperature higher than 15 C. The independent samples t-test showed that the difference was statistically significant (t(8)=-5.29, p<.05).

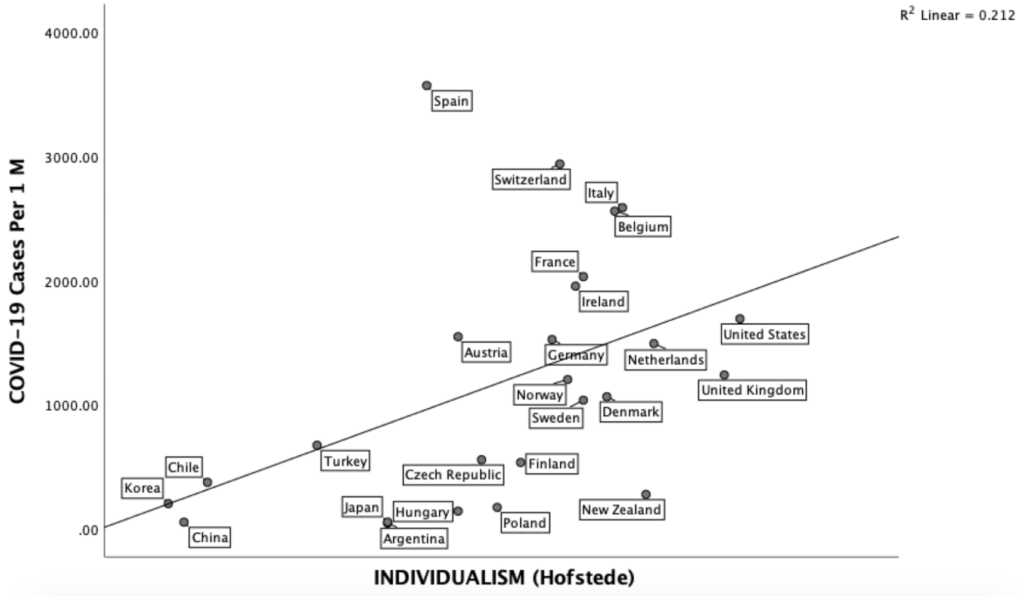
Based on the past literature, one would expect that individualism would have a negative relationship with the spread of epidemics as the members of collectivistic cultures are more likely to interact with each other which would result with higher rates of spreading the virus. However, the data shows the opposite as coronavirus cases seem to be more prevalent in individualistic cultures rather than collectivistic cultures. This on the other hand can be explained by the fact that members of the individualistic societies may not want to suppress their behavior for social distancing practices and may be less concerned about others if they have some mild symptoms. It is also known that individualistic societies tend to be more developed having more exposure to Chinese tourists, travelers and businessmen coming from the Wuhan area.

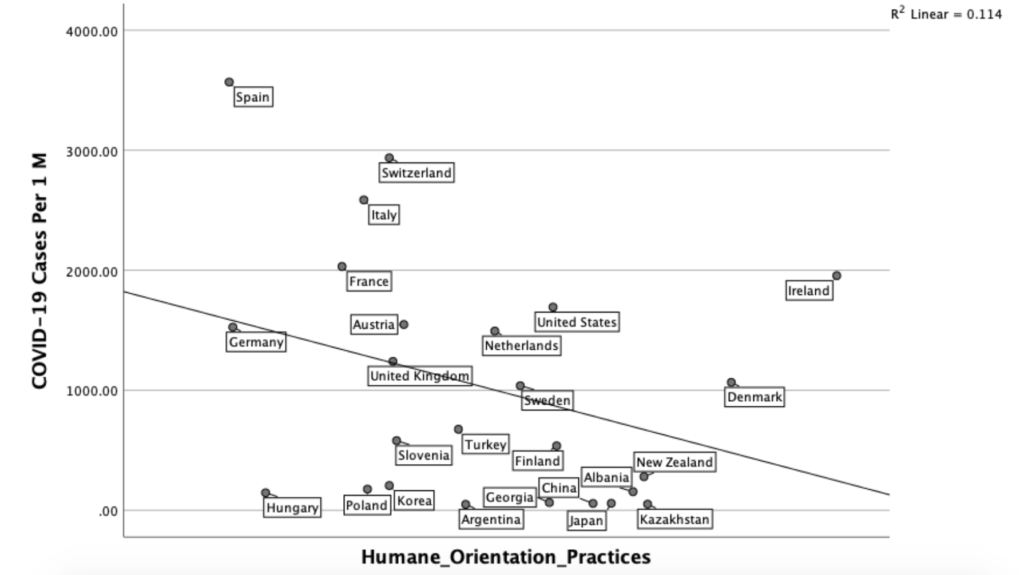
We were surprised to find no significant relationship between Hofstede’s masculinity scores and coronavirus prevalence as one would expect egalitarian and nurturing cultures to better deal with the current situation. However, we found a significant negative relationship between GLOBE’s “humane orientation practices” and the number of corona cases where “others” oriented cultures report a lower number of cases. Humane orientation stands for ““the degree to which an organization or society encourages and rewards individuals for being fair, altruistic, friendly, generous, caring, and kind to others.” ()

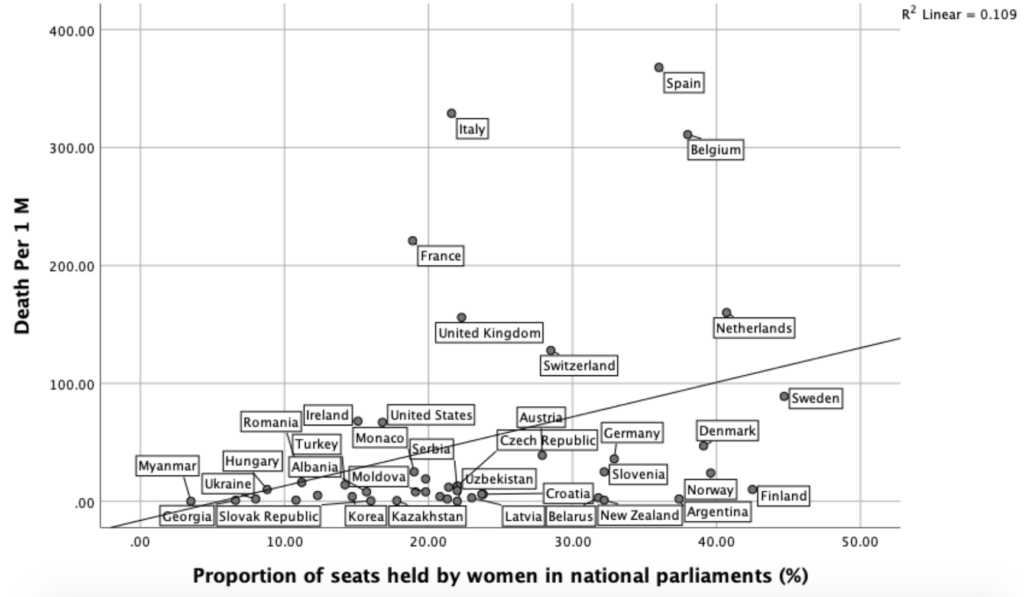
As a reflection of the “feminine culture” we looked at the relationships between coronavirus fatalities and the number of female parliament member seats. There were no significant findings that may indicate female politicians better take care of their citizens during the time of this pandemic. This finding however is only about the percentage of female parliament seats that were measured in the early 2010’s, more updated data may give a different result. Based on this finding we think the argument that female politicians are better at fighting against pandemics may be a difficult one to make.

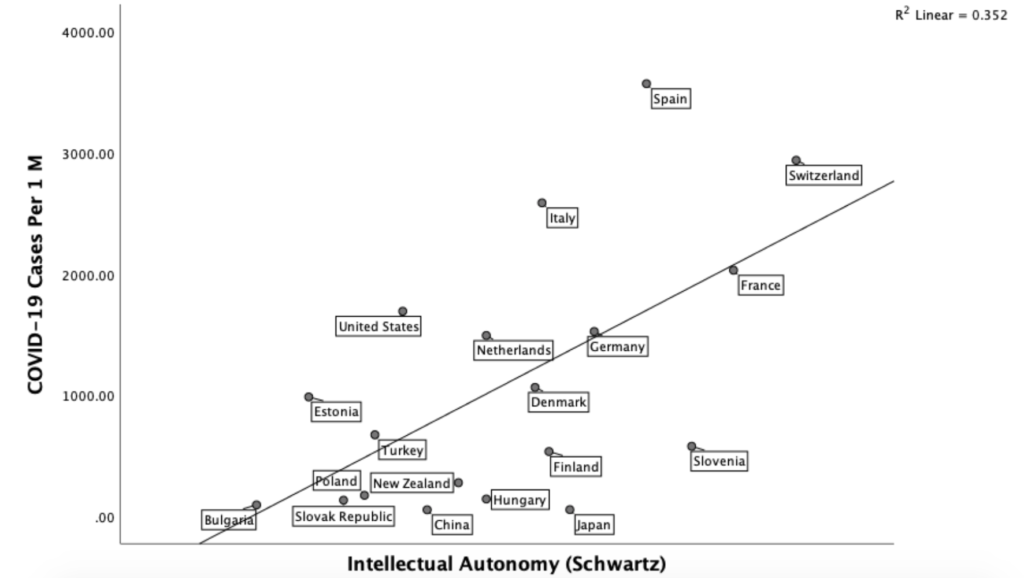
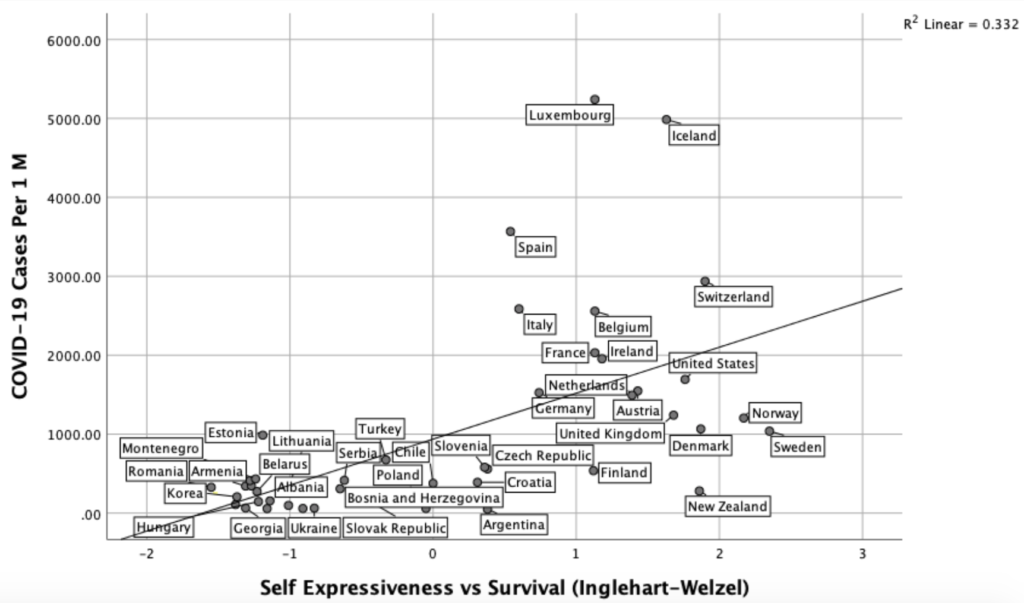
Similarly, Schwartz’ (1999) Intellectual and affective autonomy scores, which measure the country level tendencies of being open-minded and investigative, show that individualistic countries are more likely to face coronavirus cases and report more coronavirus deaths. Supporting this finding we also noticed a high correlation between Self expressiveness values (which stand for need for high quality of life and open society) and the number of coronavirus cases.


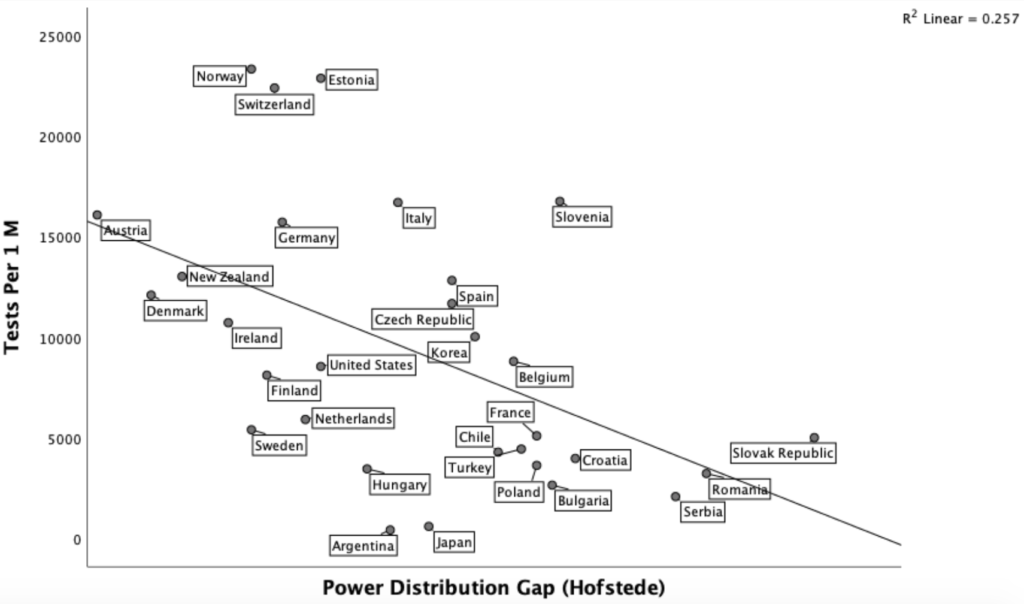
When it comes to coronavirus testing, we suspected that countries with high uncertainty avoidance and low power distance would test more. To our surprise, “uncertainty avoidance” was not related to testing but power distance was. Countries with a higher social hierarchy and possibly authoritarian regimes tested a significantly lower percentage of their citizens.

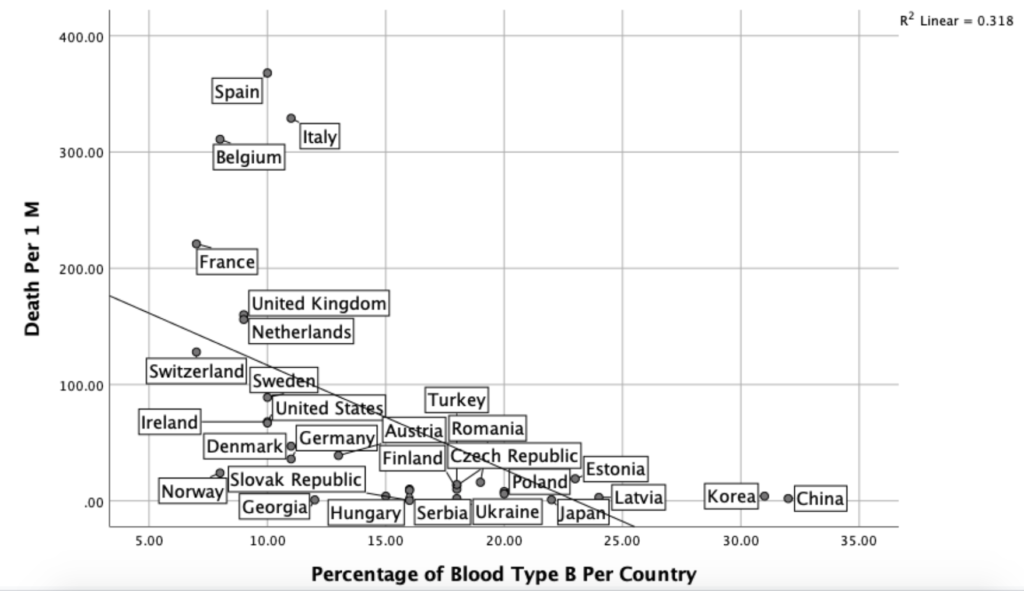
We also wanted to see if the genetic pool of each country would play a role on the number of cases and fatalities. Since it is impossible to get a single genetic code of every country, we only looked at the blood type distributions. The results showed that countries with a larger percentage of blood type 0 were more likely to report COVID-19 cases and deaths while the opposite was true for the countries with a larger percentage of blood type B. It should be noted that most countries are home to so many different nationalities with different types of blood distributions; so this finding should just be further investigated and not generalized.

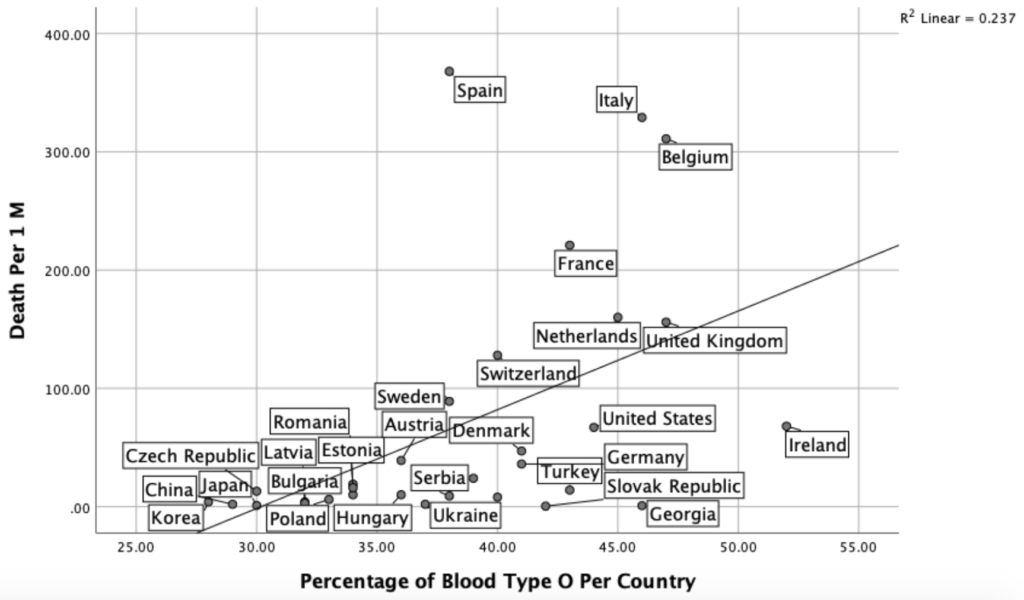

Source for the blood types ()
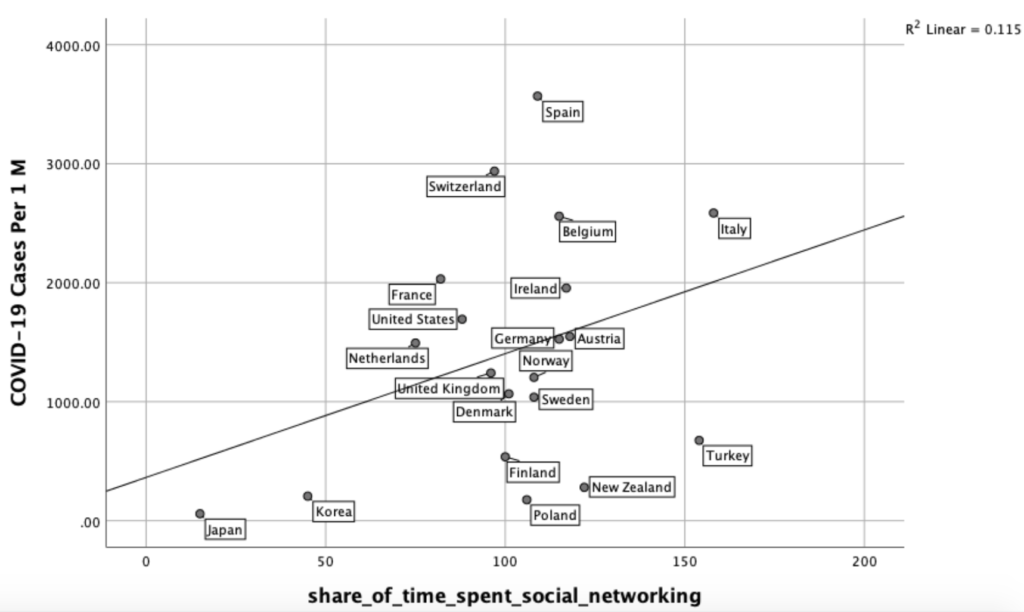
Lastly, we looked at how the use of the internet and social networks impact the spread of coronavirus and fatalities as our literature review indicated a clear relationship between culture and social media use. Our initial analysis has shown that there was a positive relationship between the spread of the coronavirus and the time-spent for online social networking. Although this finding does not make sense, since online interaction means less chances for viruses to spread, we presume that online social networking is not a substitute but a complementary tool for offline social networking. Thus, we can predict that in countries where people spend more time on Facebook, Instagram and Twitter, epidemics are more likely to spread because in these societies people are simply more “social.”

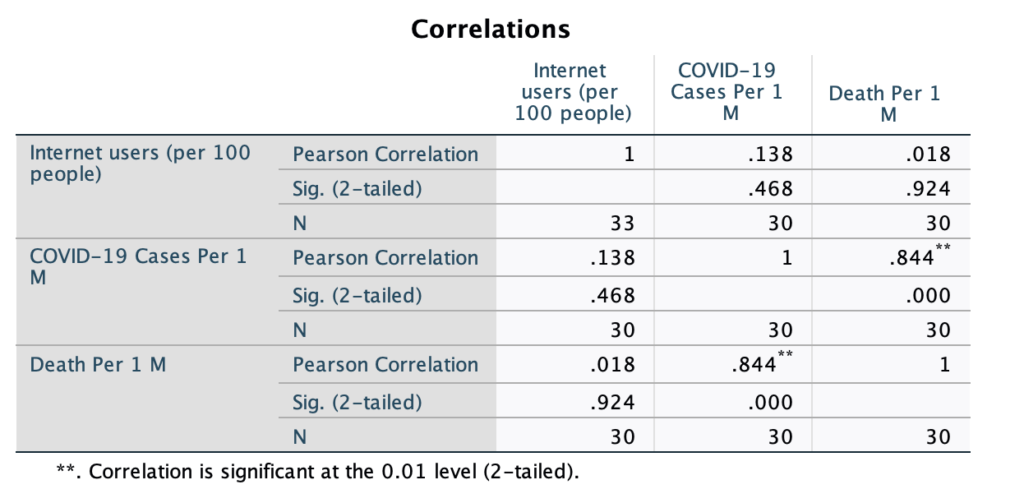
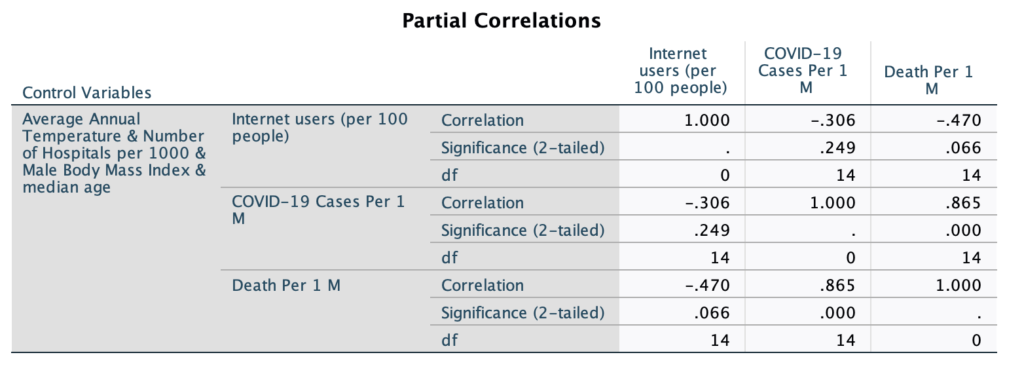
To get a holistic view, we wanted to see how the use of the internet influences the spread of the disease as people are more likely to get information about the protective measures and precautions online. Although one may expect everyone in developed countries to have access to the internet, it is a fact that a certain portion of the population has limited or no access to the internet even in high-GDP countries. Our initial analysis has shown that there was a positive correlation (Pearson) between the internet use and the number of coronavirus cases and deaths. However, when we did the analysis by controlling for the “average temperature,” “hospitals per 1000 people,” “male body bass” and “median age,” then the correlation was negative which means higher internet penetration means a lower number of casualties. See Table II and III in the Appendixes.
We provided additional analyses (smoking, BCG vaccination, correlations between country-wide diseases and coronavirus casualties, etc.) in the appendixes section for readers to consider when evaluating our findings and overall conclusions.
CONCLUSIONS
To understand the antecedents of this pandemic, we conducted some exploratory correlation tests by using the publicly available world bank data and the infections data from worldometer.com. Since there are so many confounding variables as explained in the limitations section, these findings should be taken with a grain of salt and interpreted cautiously. We provide these initial findings and discussions just to give some preliminary insights to future researchers. Our conclusions can be divided into three categories: demographic and situational characteristics, cultural factors and biological associations of coronavirus cases and coronavirus deaths as discussed below.
We first noticed that countries in warmer climates are less likely to report coronavirus cases and deaths. The results also showed that there are more coronavirus-related fatalities in countries with a high life expectancy, high male obesity and high urban population. While we found a positive relationship between GDP and coronavirus cases, we believe it is because countries in colder climates tend to have a higher GDP and people in richer countries probably had more interactions with businessmen, tourists and students from Wuhan, where the epidemic first originated.
One of the important findings in this study is that the capacity of healthcare facilities matters. There was a clear negative relationship between the number of hospital beds per 1000 people and the coronavirus deaths. This finding can help us understand why so many people in Italy and Spain, where fewer hospital beds per capita exist, died, while a relatively low number of people in Germany and Austria passed away. This is also an important finding for policy makers to consider the repercussions of large scale shut-downs as economic damages may reduce the future hospital beds per capita which is likely to cause more deaths in future pandemics.
There were also a number of cultural influences on the reported coronavirus cases and deaths. We found that there was a positive relationship between washing hands after the restroom and fewer coronavirus cases. As washing hands is one of the best ways to stop the spread of germs, this finding makes sense and may explain a relatively low number of cases in the Balkans and in Japan. On the other hand, this data is limited to European countries only, and it was a survey data; what people say and do in real life may differ dramatically. We also found no relationship between using paper money and coronavirus cases. Future studies should investigate how coronavirus prevalence in a society is related to sanitation product usage habits, bathing behavior and institutional cleanliness.
As we expected, in egalitarian societies with low power distance among the members, there was more coronavirus testing. This is probably because in those countries citizens could more easily get the testing done without the bureaucratic hassles and complicated human relationships. We could not find a relationship between “uncertainty avoidance” and mass-testing. Overall, we want to underline that the number of coronavirus deaths is likely to be a more accurate indicator of the current situation compared to the number of tests and number of cases because in general richer countries conduct more tests and thus report a higher number of cases. On the other hand, a higher number of patient check-ins may overwhelm the test conducting capacity of the countries and the case numbers may seem to decrease over time even though the opposite is likely to be true.
Individualism, not collectivism, was one of the main predictors of the coronavirus cases and deaths. Although there may be many confounding variables such as life expectancy and urbanity, we think this finding is related to concern for others in collectivistic societies and a high need for self-expression and autonomy in individualistic societies. Collective societies, where there is high social conformity and less interaction with strangers and out-group members, report a fewer number of cases and fatalities.
Perhaps the most interesting finding of this study was the clear difference between “high-contact” and “low-contact” cultures. According the Edward Hall, Southern Europeans stand closer to each other and touch more (hand-shaking, hugging, etc.) while the opposite is true for the Scandinavians and East Asians. Our data demonstrated a significantly high number of cases and casualties for South Europe (excluding warm countries) and low number of cases and casualties for East Asia and Scandinavia.
Although the main focus of this study is not analyzing biological dispositions, we detected that countries with a higher percentage of blood type O (zero) citizens reported significantly more deaths compared to countries with a higher percentage of blood type B. Even though this analysis must be done with the comparison of fatalities and recoveries within the same country we think this strange relationship must be investigated more. We also think it is worthy to explore why the same pandemic spread pattern existed for most of the major pandemics including but not limited to the Bubonic Plague, the Spanish Flu, and the H1N1 pandemic.
FURTHER NOTES ON CORONAVIRUS IN JAPAN
Recently the Japanese government was criticized for its reluctance to conduct coronavirus tests and introduce strict lock-down measures for social distancing. While it makes perfect sense to limit human interactions to reduce the spread of diseases and test citizens to assess the direction, speed and cluster centers of the epidemics, there seems to be limited literature on the effectiveness of social-distancing measures. Additionally, it is difficult to use the past methods on novel cases as each disease has a different way of spreading (e.g. Ebola virus only spreads by touching and direct contact () while coronavirus can travel in the air by 4 meters ()).
Our literature review showed that almost all the epidemics-related books point to the social-distancing measures during the Spanish Flu epidemic and not other notable cases. First well-known example is the school closures and banning of public gatherings in Los Angeles, (494 people per 100K died) vs. San Francisco (673 people per 100K died) which did not introduce swift physical distancing measures. The second example is Philadelphia vs St. Louis where in both cities a similar number of people died but the excess death rate in the early stages was way higher for Philadelphia which did not implement early social distancing measures. The problem is these examples are only from a single Western country and the past studies did not control for avg. city temperature, obesity index and hospital beds per capita all which seemed to impact the number of casualties as illustrated in our study. Additionally, the literature seems to be consistent that social distancing measures have limited effects if there are no other remedies (e.g. vaccines) and if they are not maintained for months as it is almost always the 2nd wave (). Furthermore, social-distancing measures are not cost-effective if they are not done during the early stages and in a complete manner ().
As the literature review suggests, there are likely to be differences among individuals from different societies when voluntary social distancing measures are introduced. Furthermore, not all governments may want to declare a complete lock-down right a way to combat epidemics because of the concerns of individual freedom violations in the Western cultures and the possibility of promoting voluntary behavior in high-conformity cultures. Furthermore government-forced social-distancing may sometimes have detrimental effects such as diminishing the overall public welfare and risking the health of more people than those who are in the high-risk group ().
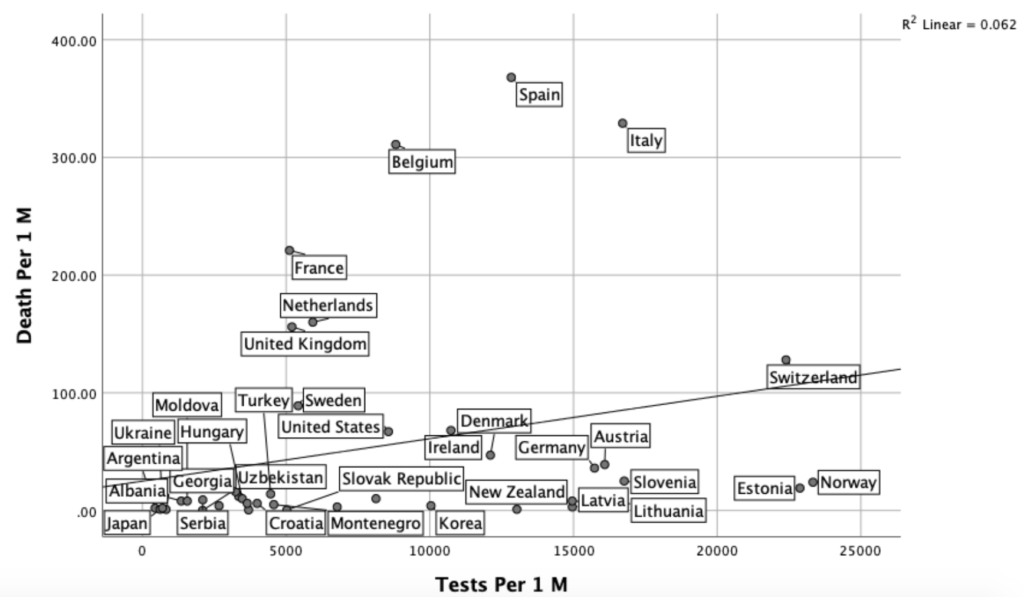
Regarding mass-testing, we could not find any data to support more tests meant fewer deaths. Although a time-series analysis is needed to conclude if tests conducted in the past reduce the casualties in the future, we expected that in countries where there are high levels of testing per 1 million population, there would be fewer deaths given the fact that four months already passed after the disease first emerged in China. Even if Japan, an outlier country, was removed from the analysis, there still was no significant relationship between tests per 1 M and deaths per 1 M. At the same time, this finding should be interpreted cautiously as when there are more cases, more tests are conducted, but, more cases also mean more deaths overall. So a positive relationship between the tests and deaths makes sense. However, the findings indicated that the relationship is probably just random. For instance Switzerland tested more people per 1M than its neighbor Austria but faced more casualties and there was a similar pattern for Norway which conducted more tests per capita but experienced a higher level of deaths per capita compared to its neighbor Finland. The same pattern was visible for the Balkan countries most of which had similar levels of fatalities but conducted different numbers of tests per capita. Future studies should investigate the time difference between the first case and the peak with its relations to the number of tests in time series analyses.

LIMITATIONS
This study is exploratory in nature and should not be used as a guideline by policy makers or practitioners because of a number of limitations.The biggest limitation of the study is the ongoing nature of the epidemic which means all the number of cases and fatality ratios are likely to change and there may be 2nd or third waves of the epidemic. Secondly, the data points in this study are the country-wide averages but most coronavirus cases tend to cluster around a small number of metropolitan areas, not homogeneously spread in every country. Similarly, most coronavirus victims tend to be males who are older than 70 but the cultural indexes or the Worldbank data represent the whole population which are likely to vary based on the gender and age groups.
Some other limitations of this study are the problems with the countrywide temperature measurement, criteria of testing and the criteria of recording fatalities. Using the avg. temperature may be misleading as summer and winter months follow a different order in the southern and northern hemispheres and many large countries have cities that experience more than 10 degrees of avg. temperature difference for any given month. Regarding the cases and fatalities, there is a risk or underreporting and undertesting. The reported case numbers totally depend on the number of candidates each country chose to test, not the actual number of COVID-19 patients. Lastly, correlation does not mean causation. Any two variables that seem to be associated in this study may be coincidentally covary or just caused by a common antecedent that should be investigated.
APPENDIXES
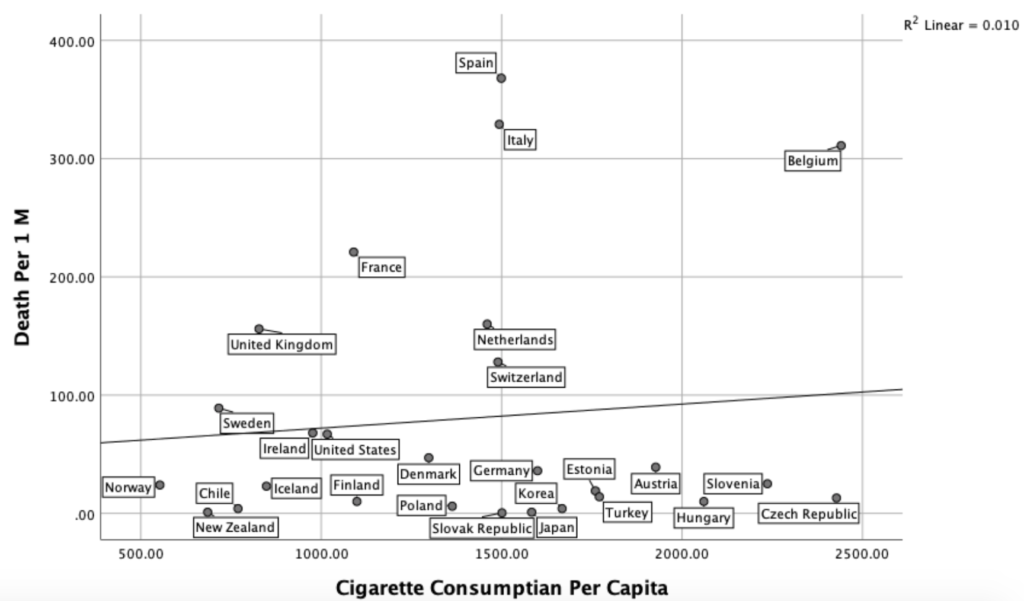
No Relationship Between Cigarette Consumption and Coronavirus Deaths
We also looked at whether the tobacco consumption habits and the prevalence of coronavirus have any relationship with the coronavirus deaths. Although these analyses must be done on the individual level, we found no relationship between the cigarette consumption per capita and coronavirus (r (49)=07, p>.05). This finding is in line with a recent finding which concluded that smoking has no positive relationship with COVID-19 casualties ().

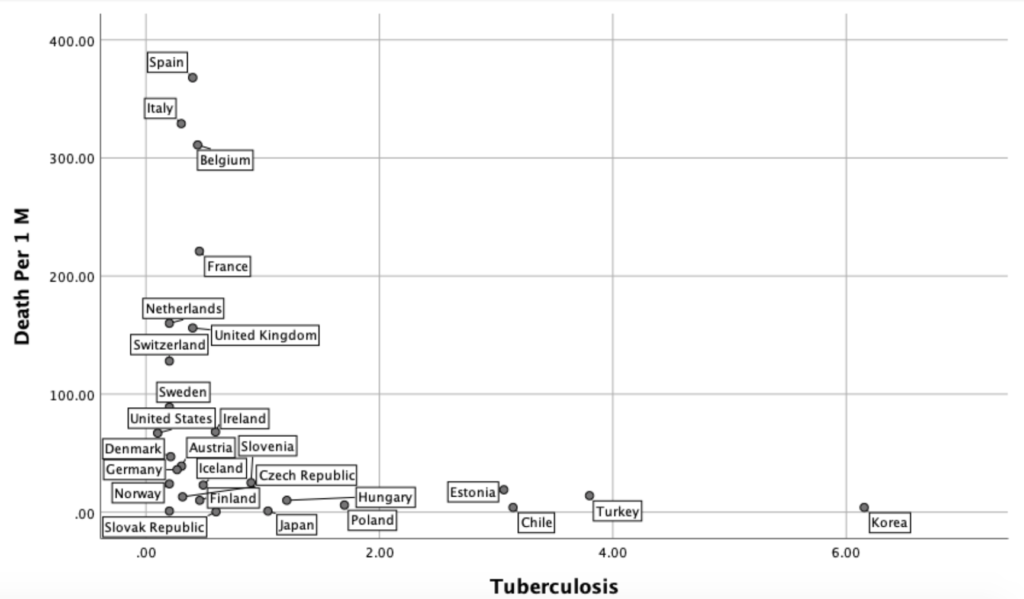
No Negative Relationship between Tuberculosis Cases and Coronavirus Deaths
When we ran a t-test analysis comparing the coronavirus death rates in countries that had no mandatory BCG vaccinations history (USA, Italy, the Netherlands, Belgium and Canada) and the rest of the world, we found a significant difference. However, since most people who die from coronavirus disease are in their 70’s who were born in the 1940s, we think this kind of comparison may be inappropriate as we have no records of BCG vaccinations from the 1940s. We expected that there would be a clear negative correlation between the current tuberculosis incidences per capita (according to WHO) and coronavirus deaths but this did not seem clear. We think it may be early to conclude that the BCG vaccine protects against the disease.

The correlates of COVID-19 Deaths
We looked at the correlations between the coronavirus fatalities and the prevalence of more than 50 diseases based on the WHO global health meta data from 2014. Readers should note that this data is the frequency of occurrence per capita, not the cause of death. Future studies should look into the relationships between coronavirus casualties and the other causes of death in each country.
Some of the notable correlates of the corona disease were iron deficiency, ischemic heart disease, and Alzheimer’s. There were more deaths in countries with iron deficiency and Alzheimer’s and fewer deaths in countries with Ischaemic heart disease and colon cancer. Interestingly there was no correlation between asthma and coronavirus deaths.

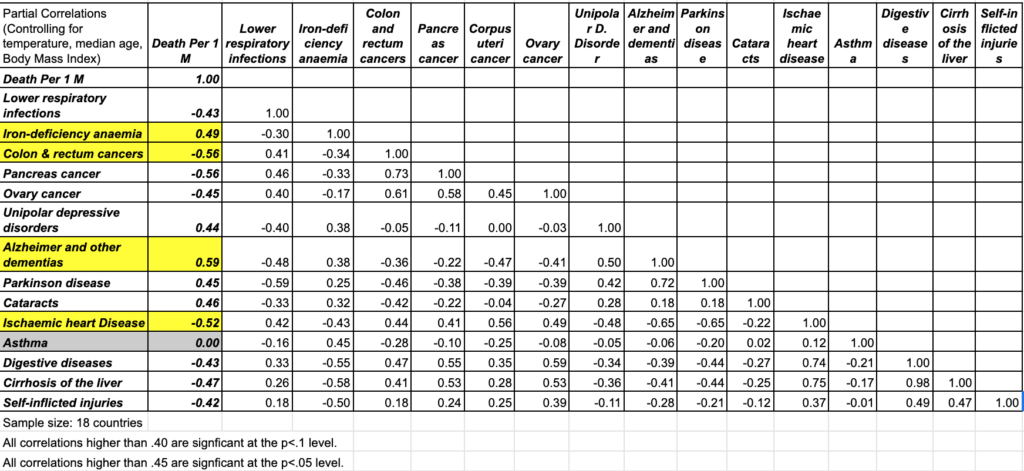


(Sample sizes are different as we had missing values for the hospital data)
REFERENCES
2012 Report, A Global Index of Sustainable Well-being, The New Economics Foundation, UK.
Abdallah, S., Michaelson, J., Shah, S., Stoll, L. and Marks, N. (2012) The Happy Planet Index
Acar, A. (2014). Culture and social media: An elementary textbook. Cambridge scholars publishing.
Acar, A. (2014). Culture, corruption, suicide, happiness and global social media use: a cross-cultural perspective. International journal of web based communities, 10(3), 357-400.
Acar, A., & Muraki, Y. (2011). Twitter for crisis communication: lessons learned from Japan’s tsunami disaster. International Journal of Web Based Communities, 7(3), 392-402.
Acar, A, Rauschnabel, P., Lin, C. and Fukui, M. (2012) ‘The relationship between personality and social media preferences’, Proceedings of the 45th Annual Conference of Japan Association of Consumer Studies.
Acar, A. (2008) ‘Antecedents and consequences of online social networking behavior: the case of Facebook’, Journal of Website Promotion, Vol. 3, Nos. 1–2, pp.62–83.
Acar, A. and Deguchi, A. (2013) ‘Culture and social media usage: analysis of Japanese Twitter
Acar, A., Takamura, D., Sakamoto, K. and Nishimuta, A. (2013) ‘Culture and brand communications in social media: an exploratory analysis of Japanese and US brands’, International Journal of Web Based Communities, Vol. 9, No. 1, pp.140–151.
Arsenault-Lapierre, G., Kim, C. and Turecki, G. (2004) ‘Psychiatric diagnoses in 3275 suicides: a meta-analysis’, BMC Psychiatry, Vol. 4, No. 1, p.37.
Average yearly temperature (1961-1990, Celsius) – by country. lebanese-economy-forum.com. Lebanese Economy Forum.
Bohret, I.The Role of Culture on Epidemic Response. Downloaded: 08 April 2020. DOI: 10.13140/RG.2.2.30525.10721
Cheng, Z. J., & Shan, J. (2020). 2019 Novel coronavirus: where we are and what we know. Infection, 1-9.
CIA World Fact Book (2013) Median Age [online] http://world.bymap.org/MedianAge.html.
comScore, It’s a Social World: Top 10 Need-to-Knows About Social Networking and Where It’s Headed, 21 December 2011, retrieved 15 November 2013 [online] www.comscore.com/content/download/12135/231287/file/Top_10_Need-to- Knows_About_Social_Networking_and_Where_it_is_headed.pdf+&cd=1&hl=en&ct=clnk.
Cook, W.A. and Pettit, R.C. (2009) comScore Media Metrix US Methodology: An ARF Research Review, retrieved 15 November 2013 [online] thearf-org-aux- assets.s3.amazonaws.com/downloads/ research/comScore-RReview.pdf.
Denti, L., Barbopuolos, I., Nilsson, I., Holmberg, L., Thulin, M., Wendeblad, M. and Davidsson, E. (2012) Sweden’s Largest Facebook Study, Gothenburg Research Institute, retrieved 15 November 2013 [online] https://gupea.ub.gu.se/bitstream/2077/28893/1/gupea_2077_28893_1.pdf.
Ellison, N.B., Steinfield, C. and Lampe, C. (2011) ‘Connection strategies: social capital implications of Facebook-enabled communication practices’, New Media & Society, Vol. 13, No. 6, pp.873–892.
eMarketer (2013) Social Networking Reaches Nearly One in Four Around the World, 18 June, retrieved 26 December 2013 [online] http://www.emarketer.com/Article/Social-Networking- Reaches-Nearly-One-Four-Around-World/1009976#HEAXV1Ujbjd9jo9o.99.
Fearon, J.D. (2003) ‘Ethnic and cultural diversity by country’, Journal of Economic Growth, Vol. 8, No. 2, pp.195–222.
G4S (2018): World Cash Report. https://www.g4scashreport.com/. Downloaded: 08 April 2020.
Grotoaert, C., Narayan, D., Jones, V.N. and Woolcock, M. (2004) ‘Measuring social capital: an integrated questionnaire in Karen Healy and Anne Hempsire’, Beyond the Local: Using Social Networks as a Policy Resource for Building Resilient Communities, The World Bank, Washington, DC.
Gutterman, A.S. (year unknown) Shalom Schwartz’s Dimensions of Societal Cultures, retrieved 15 November 2013 [online] http://alangutterman.typepad.com/files/cms—schwartzs-cultural- dimensions.pdf.
Hall, E.T. and Hall, M.R. (1990) Understanding Cultural Differences, Intercultural Press.
Hermeking, M. (2005) ‘Culture and internet consumption: contributions from cross-cultural marketing and advertising research’, Journal of Computer-Mediated Communication, Vol. 11, No. 1, pp.192–216.
Hochman, N. and Schwarts, R. (2012) ‘Visualizing instagram: tracing cultural visual rhythms’, in
Hofstede, G.H. (2001) Culture’s Consequences: Comparing Values, Behaviors, Institutions and Organizations Across Nations, Sage.
House, R., Javidan, M., Hanges, P. and Dorfman, P. (2002) ‘Understanding cultures and implicit leadership theories across the globe: an introduction to project GLOBE’, Journal of World Business, Vol. 37, No. 1, pp.3–10..
http://www.buzzfeed.com/justinesharrock/how-facebook-plans-to-make-us-all-get-along. Stravynski, A. and Boyer, R. (2001) ‘Loneliness in relation to suicide ideation and parasuicide: a
Huang, C., Wang, Y., Li, X., Ren, L., Zhao, J., Hu, Y., … & Cheng, Z. (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet, 395(10223), 497-506.
Lattin, R. and Young, S., Country Ranking: Social Capital Achievement [online] https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0CC4QFjAA &url=http%3A%2F%2Fwww.cauxroundtable.org%2Fview_file.cfm%3Ffileid%3D43&ei=Ff FGUr20EMjMkwXNqICIDA&usg=AFQjCNGXqaXgLdyAWHiNuP41E1Fk1M8clg&sig2=o 4GaAHWDr43mrS-cb88mkA&bvm=bv.53217764,d.dGI.
Levine, R.V. and Norenzayan, A. (1999) ‘The pace of life in 31 countries’, Journal of Cross- Cultural Psychology, Vol. 30, No. 2, pp.178–205.
Lippi, G., & Henry, B. M. (2020). Active smoking is not associated with severity of coronavirus disease 2019 (COVID-19). European Journal of Internal Medicine.
Markus, H.R. and Kitayama, S. (1991) ‘Culture and the self: implications for cognition, emotion, and motivation’, Psychological Review, Vol. 98, No. 2, p.224.
Martinsons, M. G., & Davison, R. M. (2007). Strategic decision making and support systems: Comparing American, Japanese and Chinese management. Decision support systems, 43(1), 284-300.
Matsumoto, D., Yoo, S.H. and Fontaine, J. (2008) ‘Mapping expressive differences around the world: the relationship between emotional display rules and individualism versus collectivism. Journal of Cross-Cultural Psychology, Vol. 39, No. 1, pp.55–74.
Phillips, H., & Killingray, D. (Eds.). (2011). The Spanish influenza pandemic of 1918-1919: New perspectives. Routledge.
population-wide study’, Suicide and Life-Threatening Behavior, Vol. 31, No. 1, pp.32–40. Thomson, R. (2013) A Socio-Ecological Approach to Privacy Concern on Facebook: The Role of
Privacy International (2007) National Privacy Ranking 2007 – Leading Surveillance Societies Around the World [online] https://www.privacyinternational.org/sites/privacyinternational.org/files/filedownloads/phrco mp_sort_0.pdf.
Rosenberg, M. (1965) Society And The Adolescent Self-Image, Princeton University Press, Princeton, NJ.
Schmitt, D.P. and Allik, J. (2005) ‘Simultaneous administration of the Rosenberg self-esteem scale in 53 nations: exploring the universal and culture-specific features of global self-esteem’, Journal of Personality and Social Psychology, Vol. 89, No. 4, p.623.
Schmitt, D.P., Allik, J., McCrae, R.R. and Benet-Martínez, V. (2007) ‘The geographic distribution of Big Five personality traits patterns and profiles of human self-description across 56 nations’, Journal of Cross-Cultural Psychology, Vol. 38, No. 2, pp.173–212.
Schwartz, S.H. (1999) ‘A theory of cultural values and some implications for work’, Applied Psychology, Vol. 48, No. 1, pp.23–47.
Sharrock, J. (2013) ‘How Facebook plans to make us all get along’, BuzzFeed, January [online]
Snowden, F. M. (2019). Epidemics and Society: From the Black Death to the Present. Yale University Press.
Toma, C.L. (2010) ‘Affirming the self through online profiles: beneficial effects of social
Trompenaars, F. and Hampden-Turner, C. (1998) Riding the Waves of Culture, McGraw-Hill, New
Tsai, W.H.S. and Men, L.R. (2012) ‘Cultural values reflected in corporate pages on popular social network sites in China and the United States’, Journal of Research in Interactive Marketing, Vol. 6, No. 1, pp.42–58.
Ur, B. and Wang, Y. (2013) ‘A cross-cultural framework for protecting user privacy in online social media’, in Proceedings of the 22nd International Conference on World Wide Web Companion, International World Wide Web Conferences Steering Committee, pp.755–762.
Wang, Y., Norice, G. and Cranor, L.F. (2011) ‘Who is concerned about what? A study of American, Chinese and Indian users’ privacy concerns on social network sites’, in Trust and Trustworthy Computing, Springer Berlin Heidelberg, pp.146–153.
Whembolua, G. L. S., Kambamba, D. K., Conserve, D., & Tshiswaka, D. I. (2015). Socio-cultural factors associated with epidemics: The case of 2014 Ebola outbreak.
World Bank (2013) Retrieved 1 September from World Data Bank Database. http://www.who.int/mental_health/prevention/suicide_rates/en/.
World Health Organization. (2013). Global epidemiological surveillance standards for influenza.
World Values Survey Group (2013) World Values Survey [online] http://www.worldvaluessurvey.org/wvs/articles/folder_published/article_base_54/files/ValueS cores_5_waves.doc.
Zhao, C. and Jiang, G. (2011) ‘Cultural differences on visual self-presentation through social networking site profile images’, in Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, ACM, May, pp.1129–1132.
Zhao, J., Yang, Y., Huang, H. P., Li, D., Gu, D. F., Lu, X. F., … & He, Y. J. (2020). Relationship between the ABO Blood Group and the COVID-19 Susceptibility. medRxiv.
Zhu, N., Zhang, D., Wang, W., Li, X., Yang, B., Song, J., … & Niu, P. (2020). A novel coronavirus from patients with pneumonia in China, 2019. New England Journal of Medicine.



Contact us : info@mai-ko.com








